Loading...

For Teenagers
- For Children
-
For Teenagers
- For Adults
- For Cleft Patients
Interception
Sometimes, it is already a bit late, before you realise that something is wrong with your child’s teeth. Putting off treatment any further may call for more aggressive treatment and/or deliver compromised results, whenever the treatment is initiated later in life.
How does early treatment help?
Orthodontic problems such as crowding of the teeth, too much space between the teeth, jaw growth problems, protruding teeth, and bad bites can be inherited or caused by injury to the mouth, early or late loss of baby teeth, or thumb sucking habits.
As a child, receiving early orthodontic treatment can help prevent the need for complicated orthodontics as an adult, leaving little to no chance of extraction or surgery in most people.
With the child in the growing phase of life, the orthodontist, if need be, can use the growth to achieve better results when treated during these years. Most children have lost all their baby teeth by age 13 and by the end of their teen years the jaw bones will harden and no longer continue to grow.
If your child is between the ages of seven and eight and shows signs of needing orthodontic care, please click here to find a Braces Specialist near your home. He/she will conduct a thorough check up and discuss with you the best steps to take towards giving your child a healthy, long lasting beautiful smile..
Early interceptive treatment is most effective for lasting results. Many of such cases need what is called a TWO PHASE treatment.
Two phase treatment
Two-phase orthodontic treatment is a specialized process combining tooth straightening and physical, facial changes. The purpose of two-phase treatment is to maximize the opportunity to accomplish the ideal healthy, functional and aesthetic result that will remain stable throughout your life.
Phase – One
The goal of Phase-One treatment is to help the jaw develop into a better position, and make maximum space available to accommodate all of the permanent teeth and improve the way the upper and lower jaws fit together.
It involves limited orthodontic treatment utilizing growth modification appliances, expanders, arch developers, myo braces, trainers, partial/limited braces before all of the permanent teeth have erupted. Such treatment can occur between the ages of 7-11 years and usually last 10-15 months
Phase 1 treatment lays down a good foundation for the erupting permanent teeth and corrects growth/jaw problems that would otherwise require complex and extensive treatment later. Receiving early treatment may prevent the removal of permanent teeth later in life, or the need for surgical procedures to realign the jaws.
Resting Period
In this phase, the remaining permanent teeth are left alone as they erupt. A successful first phase will have created room for permanent teeth to find an eruption path. At the end of the first phase of treatment, teeth are not in their final positions. This will be accomplished in the second phase of treatment. Selective removal of certain primary (baby) teeth may be in the best interest of enhancing eruption during this resting phase. Therefore, periodic recall appointments for observation are necessary, usually on a six-month basis.
Phase – One
The goal of the second phase is to make sure each tooth has an exact location in the mouth where it is balanced with the lips, cheeks, tongue, and other teeth. When this equilibrium is established, the teeth will function together properly. Phase two usually involves full upper and lower braces.
The second phase begins when almost all permanent teeth have erupted. Retainers are worn after this phase to ensure retain the healthy beautiful smile achieved.
Dentofacial Orthopaedics
Dentofacial orthopedics involves the guidance of facial growth and development, which occurs largely during childhood. Dentofacial orthopedics is the process of “normalizing” the growth and position of a child’s jaws and minimizing any imbalances of the face and jaws.
Children are often the best candidates for dentofacial orthopaedics. 9-11 years of age is a period of significant growth in most children and it is important to take advantage of that growth in children who have certain types of bite problems:

Lower jaw and teeth too far behind the upper teeth when biting together (overbite)

Upper back teeth too narrow compared to the lower teeth when biting together (crossbite)

Upper front teeth behind lower front teeth when biting together (underbite)
Appliances are used for this treatment:
- Myofunctional appliances like Activator, Bionator, Frankel’s appliance or Twin block appliances which harness forces from child’s jaw musculature to redirect jaw growth.
- Phase 1 fixed braces called 2 x 4 appliance to normalize alignment of erupted permanent teeth which help remove the impediments in the developing jaws
- Palatal expanders for cross-bite correction.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Please note – each and every case is unique and it is the Orthodontist’s diagnosis and treatment planning that will decide the type of appliance most suited to deliver the best possible result in a particular case.
Habit Correction
It’s quite normal for a newborn child to put hands, fingers and other things in his/her mouth. As the child grows bigger he/she may develop a habit to suck their thumb, fingers, hand, or put other inanimate object such as a blanket or toy in the mouth. Most children discontinue their nonnutritive habits between the ages of 2 and 4 years.
However few continue it for a longer period of time and develop dentally deleterious habits
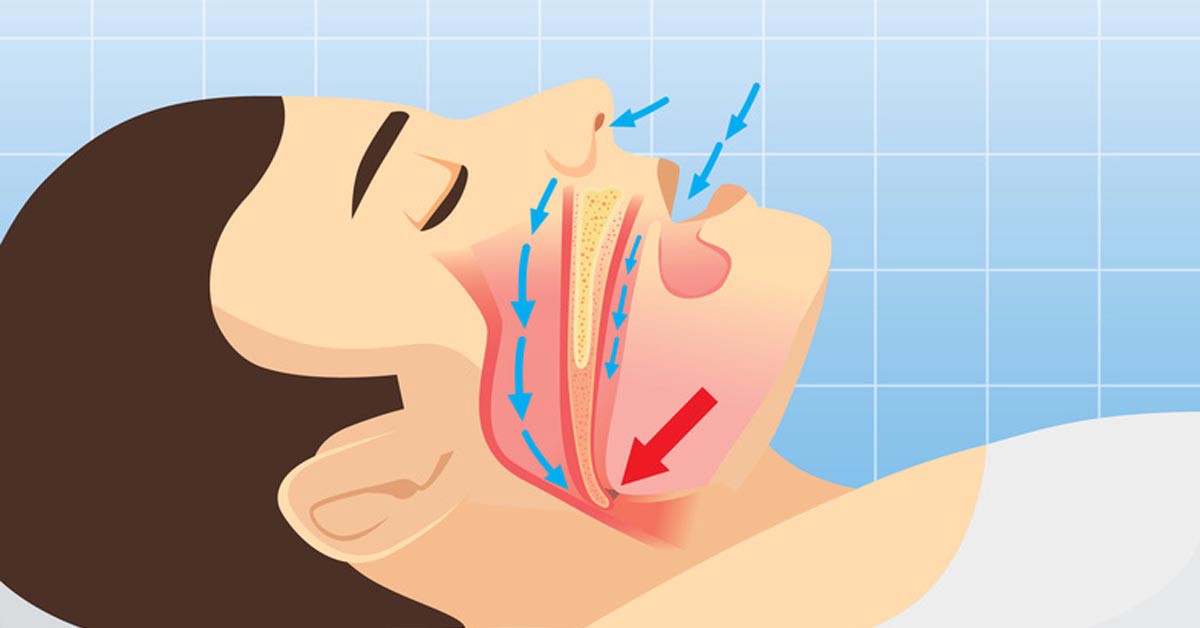 mouth breathing |
 thumb sucking |
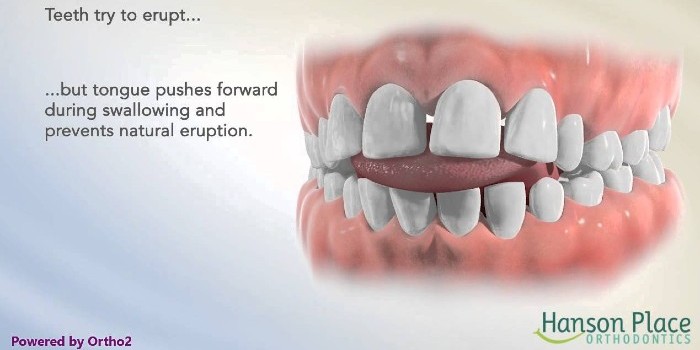 Tongue Thrusting |
|
lip sucking |
The dental effects of various oral habits directly correlate with the frequency, intensity, duration, and nature of the habit. Continuous application of suction forces by children causes the cheeks to place inward pressure on the upper teeth, which Leads to narrowing of the palate, posterior crossbite (reverse overlap of the upper and lower back teeth), and incisor protrusion (an outward flaring of the child's upper incisor teeth). Often the lower incisors will tip toward the tongue as well (incisor retrusion). This increases the child's overjet—the horizontal distance by which the upper incisors overlap the lowers, and increases the likelihood of the child chipping or otherwise injuring a front tooth.
Because such children spend a significant amount of time with objects between their front teeth, the back ones frequently erupt farther than normal (passive eruption). When this happens, the child's front teeth may no longer overlap vertically, a condition known as an anterior open bite. The child's speech development may be affected in such cases, as well as their ability to chew properly.
Dental effects are generally reversible and unlikely to cause any long-term problems if the habit is discontinued by the age of 5.
In some children, the oral habit persists despite reasonable attempts to discourage it. It may be necessary in such cases to place a habit appliance on the teeth of such children—a gentle reminder to the child not to place fingers, thumbs, or other objects into their mouth. Examples of such appliances are PALATAL CRIB, ORALSCREENS, which are completely passive device (does not move teeth or jaw bones), yet is an active means of discouraging the habit; the appliance is removed after the habit is broken.
{kind=link}
{kind=link}
Correction
Quite often, the parents fail to notice a developing malocclusion and visit an Orthodontist only after the teeth have gone totally out of alignment. By 12 years of age, more often than not, all of the permanent teeth have erupted and crooked teeth, gaps between the teeth and bad bites become very obvious. Children, who would otherwise be very reluctant to wear braces, do not mind having it, because they see their friends wearing them, too, and want to fit in. Orthodontists can usually take advantage of the growth spurts which happen around this age, to help shape the bite and teeth correctly.
A wide array of appliances are available to deliver the most stable, functional set of teeth which would present the most good looking smile. Click here to know about the different types of braces. The knowledge and skill of the Orthodontist will help determine, which of those are most suitable for a particular case.